Commentary on “Arachnoid cysts of the quadrigeminal cistern: Proposal of a therapeutic algorithm based on a systematic review of literature”
DOI:
https://doi.org/10.46900/apn.v5i3.198Keywords:
quadrigeminal cistern, arachnoid cysts, endoscopic third ventriculostomy, neuroendoscopy, hydrocephalusAbstract
Quadrigeminal plate arachnoid cysts (QACs) usually raise a great interest among neurosurgeons, especially those dealing with children, because of the peculiar location (midpoint of the intracranial space), the surrounding anatomy and the possible clinical implications (rich number of possible signs and symptoms, hydrocephalus).
As for most of the other types of arachnoid cysts, QACs are treated by an endoscopic fenestration in many Centers since it is felt as the best approach to manage them and the associated hydrocephalus. However, according to the literature, there is not enough evidence to recommend this approach because of the rarity of QACs and, subsequently, the low number of dedicated studies. Actually, microsurgery and even shunt are still advocated as effective though burdened by a higher rate of complications [1].
On these grounds, the review performed by Ferreira Furtado and coworkers provides a relevant update to increase the knowledge about QACs. First of all, a careful analysis of the anatomy of the quadrigeminal plate region, namely its anatomical limits and the differentiation of its arachnoid complex, allows to understand why ovoidal-shaped QACs mainly grow following an antero-posterior path without causing aqueduct compression while the globular-shaped ones mainly grow along a rostro-caudal axis resulting in aqueduct stenosis and hydrocephalus. These findings, which can be commonly found in the daily clinical practice, have important implications on the prognosis other than on the indications for surgery.
Secondly, this review study further supports neuroendoscopy as the gold standard way to manage QACs. In the personal experience, a ventriculociststomy plus cisternostomy or ETV is realized whenever possible to increase the success of the endoscopic procedure, independently from the age of the patients [2-4]. Good results are reported even in infants old less than 6 month [5,6]. Actually, the risk of reoperation after neuroendoscopy for QACs is related only partially to the young age of children since it can result also from a misdiagnosed/not properly treated hydrocephalus [7].
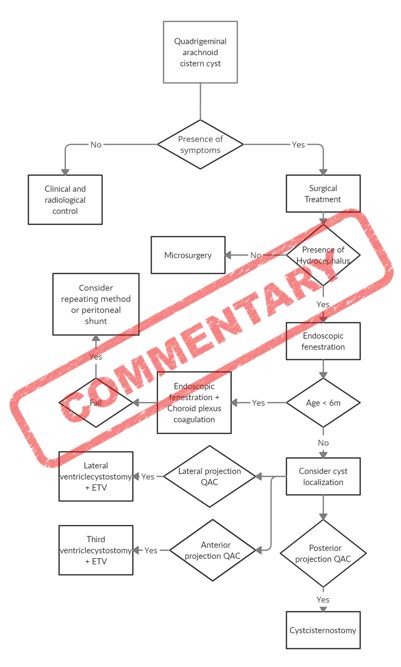
The proposed algorithm of treatment is shareable for several reasons: 1) It shows no need of surgical indications in asymptomatic cases with radiologically stable QACs. Indeed, the ovoidal-shaped cysts, in spite of an initial growth that can occur in the first months of life, tend to remain stable in size and asymptomatic; 2) It demonstrates the predominant role of neuroendoscopy in the management of QACs, especially when hydrocephalus is associated, by confirming its safety and effectiveness. Indeed, microsurgery maintains a role in selected case, that is when a reliable fenestration cannot be obtained through the endoscopic approach. Actually, due to the invasiveness of the supracerebellar infratentorial or the suboccipital transtentorial route, the routine use of microsurgery is discouraged [8]. Similarly, shunting procedures should be adopted only in case of repeated failures of the previous techniques. Also the advantages on the long-term outcome of fenestrating the cyst into the cistern (interpeduncular cistern by ETV or ambiens cistern by cisternostomy) rather than into the lateral ventricle only is reaffirmed.
The only questionable point of the algorithm is the use of “endoscopic fenestration + choroid plexus coagulation (CPC)” in infants < 6 months. Actually, CPC has been demonstrated to increase the success rate of ETV in infants, although the results are mainly limited to the Uganda and USA experiences, but such a success is the result of the association between CPC and ETV and not from CPC and cyst fenestration [9]. Therefore, such an option should be proposed in infants with QACs and hydrocephalus manageable with ETV. Moreover, since CPC adds some risks of morbidity to the endoscopic procedure (ETV + cyst fenestration), at least ad adequate ETVSS (ETV success score) [10] should be reached by the patient prior to consider an ETV-CPC in addition to the mere cyst fenestration.
As acknowledged by the authors, the main limitation of this study is related to the rarity of QACs and, subsequently, to the few studies and cases available on the literature. However, their analysis provides an updated view on the current management of QACs. Moreover, it could represent the trigger to propose a multicenter study.
Downloads
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2023 Luca Massimi

This work is licensed under a Creative Commons Attribution 4.0 International License.

When publishing in Archives of Pediatric Neurosurgery journal, authors retain the copyright of their article and agree to license their work using a Creative Commons Attribution 4.0 International Public License (CC BY 4.0), thereby accepting the terms and conditions of this license (https://creativecommons.org/licenses/by/4.0/legalcode).
The CC BY 4.0 license terms applies to both readers and the publisher and allows them to: share (copy and redistribute in any medium or format) and adapt (remix, transform, and build upon) the article for any purpose, even commercially, provided that appropriate credit is given to the authors and the journal in which the article was published.
Authors grant Archives of Pediatric Neurosurgery the right to first publish the article and identify itself as the original publisher. Under the terms of the CC BY 4.0 license, authors allow the journal to distribute the article in third party databases, as long as its original authors and citation details are identified.